I started on Ivabradine just over a month ago with a slow start of 2.5mg bd (twice a day) and have now increased to the 5mg bd. Is it working? Well, it’s doing something, that’s for sure. But I’m a bit surprised it isn’t doing as much as I expected.
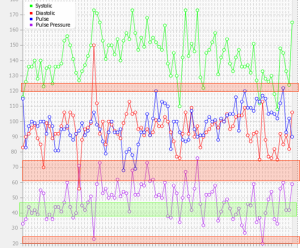
The top red band shows a POTS tacky level ie. above 120 and you can see I don’t often get there now. This is good. However, I do seem to have more bouts of sitting still severe palps over 130 in the evening or in bed at night (not on chart) Nevertheless overall I think my heart rate is down. I’ve even had a few in the 70s. Very nice.
No obvious side effects so far which is good. My breathing is rubbish and I did come off the Ivabradine for a few days to see if it was the culprit but nothing changed other than my HR going up. Having seen the GP I’m back on the Ivabradine and putting up with the breathlessness which a dose of steroids hasn’t helped. Weird, because they usually do.
I have been surprised at the lack of real impact on my resting pulse. It’s down from 110 on average to around 97 but it’s often 100 or over 100 still. So the real impact has been on my upright heart rate which is so much better. I assume the Prof will increase the dose when I get to see him (I think the usual dose is 7.5mg bd).
The GP has adjusted my Candesarten 4mg and 8mg from just 8mg. My BP remains as fluctuating as ever. It’s sometimes great and sometimes high even when I’m sitting still. Moving around sends it upwards very sharply along with sudden drops. Not nice at all. I still think this is orthostatic in nature.
The numbers at the bottom, in purple, are my pulse pressure. As you see it’s rarely in the green. It is generally too high and too often it’s way too high.
I am glad the GP took seriously my report of a TIA last month (about 6 weeks ago) as fluctuating BP along with such high numbers on pp are a bit concerning. Strangely research so far shows that people over 60 can safely cope with PPs as high as 70 but people under 50 don’t do so well. The research is extremely thin on the ground.
From Dys.Girl I am hoping to join the pulse pressure research group. I am pretty sure the wildly fluctuating BP and even tacky levels are because my ANS is bust, but without proper research the “what now?” can’t really be answered.
I am awaiting bloods and of course the wait for standing norepinephrine and dopamine levels. I really want those done because I am still thinking along hyper or comboPOTS lines, especially as my BP is so high when I stand up. I am assuming the bloods I’m having taken next week will cover things like full blood count, cardiac enzyme and BNP but I’ll have to ask when I get there.
I also think I might want to get ANAs done in case of Lupus now that I am the less than proud owner of a malar rash. (butterfly rash). It comes and goes and ranges in colour from purple to bright red. As the tests for Lupus are notoriously unreliable I am unsure whether to bother asking for them now. It would only be useful if there was a proper treatment – and I am not so sure there is.
Multicoloured bodily features are continues with red knees and blue feet in the mornings. All very Dulux of me I think. Also keep having Oxygen SaTs below 93 sometimes hovering around 90-91. No wonder I feel a bit off.
Wish it was all simple. But on the other hand, it’s like a detective story sorting through all the clues; even if it is unfortunate that it’s my body doing this.